.jpg)
A Short Update of Frankel Functional Regulator
Lakshmi Thribhuvanan* , M.S Saravankumar and G Anjana
1Department of Pedodontics and Preventive Dentistry, Royal Dental College, Iron Hills, Chalissery, Palakkad, Kerala, India .
lakshmithribhuvanan91@gmail.com
http://dx.doi.org/10.12944/EDJ.03.01.03
A removable appliance is a device that modifies mandibular posture and transmits the resultant forces created by muscles and soft tissues to underlying and surrounding anatomical structures in a controlled manner. The resulting variation of the neuromuscular environment thus produces the required tooth movement along with the needed advancements in growing patterns. The necessity and requirement of early treatment is to modify the existing and developing malocclusions and muscular derangements before the attainment of growth completion of permanent dentition. Frankel Function Regulator (FR) is a device which functions on the principle of functional orthopedics in unity with muscle gymnastics (muscle exercises) and thereby results in morphological changes in both the jaws hence re-establishing the desirable normal occlusion.
Copy the following to cite this article:
Thribhuvanan L, Saravankumar M. S, Anjana G. A Short Update of Frankel Functional Regulator. Enviro Dental Journal 2021; 3(1).
DOI:http://dx.doi.org/10.12944/EDJ.03.01.03Copy the following to cite this URL:
Thribhuvanan L, Saravankumar M. S, Anjana G. A Short Update of Frankel Functional Regulator. Enviro Dental Journal 2021; 3(1). Available From: https://bit.ly/3k3Fw9J
Download article (pdf) Citation Manager

Introduction
Facial esthetics play a pivotal role in the perception of beauty.1 According to AAPD (American Association of Pediatric Dentistry) growth and development of dentition is an important aspect taken into consideration to provide oral health care for all pediatric patients. This established guidance should thus result in the development of permanent dentition which is functional with an acceptable and esthetically coherent occlusion.2
Edward Hartley Angle stated that the absolute designing of a normal function causes the craniofacial structure subsequently to follow this pattern.1 Hence malocclusion is the consequence of various skeletal and dental functional derangements.3 It is important to identify whether this resultant cause of malocclusion is skeletal, dental or functional.4 The treatment modifications and plan of the resulting skeletal problems include:
- Growth Modification Treatment- Head gears
- Functional Appliances Treatment -Dental Camouflage
- Fixed Appliances and
- Orthognathic surgery.
In growing patients all of these varied treatment modalities can be utilized while in adults the choice of treatment is comparatively limited and restricted to very few selectable approaches.5 The greatest advantages of functional appliances when given during the pubertal growth phase is that they can rectify both dental and skeletal discrepancies in all the three planes of sagittal, vertical and transverse directions thereby giving an acceptable treatment outcome for parents as well as the child.6 Function Regulator appliance is the most commonly used tissue borne appliance which is named after the inventor Rolf Frankel.3
Historical Preview
The Activator appliance which was developed by Viggo Andresen which helped in mandibular advancement resulted in a biomechanical force, thereby restricting the mandible to attain back to the previously established position.7 The extreme complexity and heaviness of the activator to wear during night prompted Balters to modify it in 1960, and he called it the Bionator.8,9
 | Figure 1: Rolf Frankel Click here to view Figure |
The most remarkably significant modification and development in removable appliances innovations was the Funktionsregler (Function Regulator) of Rolf Frankel (Fig1) in 1967. The Function Regulator (FR) was constructed to act as an adjunct device with exercise as its major function of purpose. Its mechanism of action was mainly based on combination of existing rules of orthopedics, muscular exercises & timely muscular trainings. These were considered as the chief factors in development of osseous tissues. Frankel strongly advocated that poor postural behavior of the orofacial musculature resulted in Class II malocclusions.
Physiology of Orofacial Complex
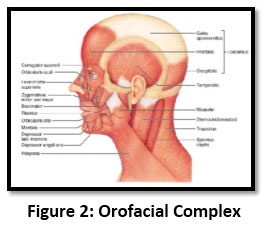 | Figure 2: Orofacial Complex Click here to view Figure |
During post-natal development, muscular movements progressively have an alternating impact the developing functional space. During swallowing, (Fig2) air in oral cavity is expelled into pharynx and thus resulting vacuum is established. When the mandible is manifested into rest position, this results in diminution in the existing atmospheric pressure which takes place in inter-occlusal space.
The muscular forces and sub-atmospheric pressure present in the oral cavity exerts excessive unbalanced pressure on labial teeth surfaces. This force thus causes to suck the lips & cheeks against the teeth. This supplies the missing enigma in the concept of equilibrium theory.
The airflow all through inspiration is the consequence of diminished air pressure within the respiratory tract. During expiration the elasticity of extended tissues returns the thorax to its normal size causing pulmonary air compression. The pressure exceeds beyond the atmospheric pressure & air flows out from the lungs.
Thus in establishing the physiological conditions in the orofacial area, utmost imperative adapted biomechanical methodologies & aspects are as follows: 11
- Physiological spaces in the oral cavity & in nasopharyngeal spaces.
- Postural performances maturation of orofacial muscular capsule during childhood.
- Defect less functioning of valves in orofacial region with establishment of a competent oral seal.
Advantages of Function Regulator
- Removal of abnormal muscular activity and promoting normal development pattern.
- Treats skeletal malocclusion.
- It plays an important role in prevention and correction of oral habits.
- Treatment can be initiated at an early age and is most often started in the mixed dentition period.
- As the treatment is started at an early age, psychological disturbances associated with malocclusion can be avoided.
- Provides incisal capping which reduces risk of damage to front teeth in the presence of forwardly placed front teeth.
- The mentioned appliances are manufactured in the dental laboratory thereby indicating less chair side time for the patients treated.
- The frequency of the patient’s visit to the orthodontist is less than in case of fixed or removable appliances.
- It does not interfere with oral hygiene maintenance.
- Less expensive than fixed appliances.12
Disadvantages of Function Regulator
- These appliances are functionally allied to cause extrusion of maxillary and mandibular molars.
- Removal of overbite can result in increase in lower anterior facial height
- Unwanted tooth movements of rotation and translations are obtained along with establishment of functional occlusion.
- The treatment outcomes are reliant on patient’s level of comfort and experienced cooperation.
- Limits their application in non-growing adults and in treatment of horizontal discrepancies.
- Their application cannot be used to bring about single or unique tooth movement or changes.
- Most functional appliances are dependent on the patient for timely wear which justifies the necessity of patient cooperation essential for the success of the treatment.
- These appliances have detrimental side effects on the position of the front teeth.
- Speech may be strongly malfunctioned.
- The treatment with functional appliances takes longer than with established fixed functional therapy.12
Frankel Philosophy
Rolf Frankel establishes that the tongue plays an imperative role in outward growth of teeth and surrounding tissues. These effects have been overestimated to the exclusion of buccal musculature. Majority of the tongue function may be compensatory to dentoalveolar morphology and may not be the primary cause of the pre-existing malocclusion and development.13The anterior lip seal and a posterior oral seal provided by the tongue and soft palate during deglutition process, produces a negative atmospheric pressure occurs in the oral cavity. The cheek muscles are then sucked into the interocclusal space as the mandible returns back to the postural rest position in the final phase of the swallowing. The effect is both a contracting effect on the dentoalveolar process and prevention of eruption of the buccal segments which then interposed the cheek tissue. The partial vacuum created inside the arch creates more external pressure, thereby removing the intrinsic force potential of the tongue tissue. The FR buccal shields prevent the pressure of the buccinators mechanism on the dentoalveolar as of both during deglutition and at rest. The net result is outward expansion to the “ought to be” acrylic shield functional matrix.
The labial wire of the Frankel appliance rests on the maxillary incisors, but is not activated or “pinched-up” as with Hawleys appliance. This determined action tips the incisors excessively to the lingual alveolar plate. It restricts the full mandibular horizontal growth in the deep bite and the upper anterior segments applying a controlled retracting effect on mandibular incisors and the entire mandible when the appliance is not worn regularly. Apart from preventing the deforming muscle action and allowing the teeth to erupt down and outward, the shields and pads are extended into the vestibular depths, putting the defined tissue under tension without creating any local tissue irritation. This tension exerts a pull on the periosteal tissue of the maxillary bone. The degree to which the significant expansion is caused by periosteal pull is conjectural at this specified point. The vestibular constructions act as a base for oral gymnastics exercises performed by the patient. The stability of the results achieved by the FR was thus interpreted as connected with a change in the oriental muscular balance and the establishment of a newly developed and modified muscular balance.
Parts of Function Regulator
Function Regulator I (FR-I)
 | Figure 3: Function Regulator I Click here to view Figure |
It (Fig3) is composed of two shields on buccal surface, two pads on labial surface, another pad on lingual surface with associated wire parts which form the component parts of FR-I.
- Acrylic Parts
Buccal Shields
These shields are placed deep into buccal sulcus in relation to maxillary first bicuspid and associated with the tuberosity of maxilla. The shields must be placed at an ideal distance from lateral aspects of the respective teeth & corresponding alveolar ridge where dentoalveolar expansion is required. The thickness of these shields should not be more than 2.5mm.
Labial Pads
These are rhomboid shape, occupies the facial surface of lower alveolar process. The anterior edges of lips pads should be placed at an ideal distance of 5mm from the gingival margin. The posterior edge of the pads should be limited to the facial canine protuberance which would otherwise cause mucosal irritation of lower lip and hindrance in speech.
Lingual Shield
This occupies the position below gingival margin of lower teeth & flares out posteriorly to the roots of lower second bicuspids.
- Wire Parts
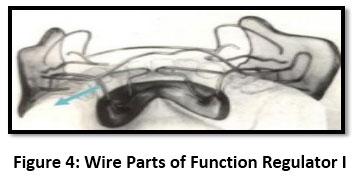 | Figure 4: Wire Parts of Function Regulator I Click here to view Figure |
Vestibular Wires
These are the parts (Fig4) which are not embedded into the acrylic. They should be placed at the outer surface of the alveolus not extending beyond 1½mm. They have to be bent to engage into the depressions of the alveolar processes on their facial surfaces.
Labial Wire
This occupies the central portion of the facial surface of the maxillary incisors & runs gingivally at right angle between the roots of lateral incisor & canine. It curves distally at the centre of the canine’s root.
Palatal Bow (Pabo)
This bow transverses the palate with an arch bend in the posterior direction and runs interdentally between maxillary first molar and second bicuspid. This makes a loop into buccal shields which emerges to form an occlusal rest. This occlusal rest prevents displacement in vertical direction.
Canine Loop
The canine loop is locked in buccal shield at the occlusal plane and steeply goes to the gingival margin of the maxillary first bicuspid. This runs parallel to the lingual surface of the canine for 1mm and transverses the interproximal contact existing between the canine and lateral incisor.
Two Lower Lingual Wires
These two wires are attached to the lingual shield and passes along the lingual surface of incisors at cingulum. Their function corresponds to protracting of the mandibular incisors.
Crossover Wires
These wires connect the lingual shield with the buccal shield. These should not impinge interdentally in mandibular advancement.
Function Regulator II (FR-II)
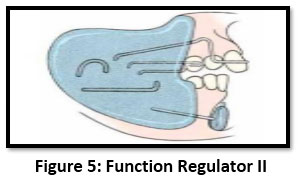 | Figure 5: Function Regulator II Click here to view Figure |
FR-II (Fig5) differs in structural formulation from FR-I only by the addition of an upper lingual wire and an additional amended canine loop. These wire components originates from the shields of buccal surface and runs to engage between the maxillary canine and the first bicuspid.13
Function Regulator III (FR-III)
FR-III (Fig6) consists of shields on buccal surface as the conventional design, two upper lip pads along with numerous wires. It appears as an FR-II turned upside down but there exist constructional differences.13
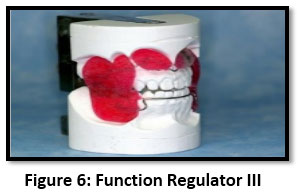 | Figure 6: Function Regulator III Click here to view Figure |
Acrylic Parts
Buccal Shields
They are placed from maxillary dentoalveolar process expanding the circumoral capsule in lateral direction within 2.5 mm from the alveolar ridge and 3 mm from the teeth surfaces. Lateral dimension permits transverse development of maxillary dentoalveolar structures.
Lip Pads
They are dimensionally larger than that of FR-I and FR-II and are protracted far into the sulcus. They should be parallel and should be precisely away from the alveolus by 2. 5mm in distance. The functional advantage of projecting lip pads and superior portion of the buccal shields is to expand the orofacial capsule and aid in growth and development.
Wire Parts
Palatal Bow
This bow connects the two shields on buccal surface and locks the appliance against the contracting forces of circumoral musculature.
Upper Lingual Wire
The action of this wire is retracting the proclined maxillary incisors. The palatal bow and upper lingual wire has to be curved so as not interfere with the occlusion. The palatal bow runs distally to the last maxillary molar & the lingual wire acts as a crossover wire.
Lower Labial Bow
This should provide a firm contact with the mandibular incisors and canines.
Occlusal Rests
These are place on last mandibular molar for correcting an anterior cross bite. In most of cases this expansion with the occlusal rest is enough for maxillary incisors to move incisally.
Function Regulator IV (FR-IV)
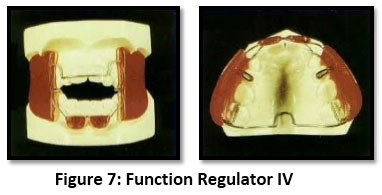 | Figure 7: Function Regulator IV Click here to view Figure |
The FR-IV (Fig7) has two shields on the buccal surface similar to the normal architecture, two pads on lower lip surface, a palatal bow, a maxillary labial wire and four occlusal rests. Buccal shields and mandibular labial pads carry out the same function similarly to that of FR-I and FR-II. The mandibular lip pad restricts hyperactive mentalis muscle and trains the lip to attain a definitive anterior lip seal. The labial bow is used to rectify the protruded maxillary incisors. The occlusal rests should engage on the occlusal surfaces of the maxillary buccal teeth. The palatal bow should occupy the space behind the distal most molar favouring a dorsal directional shift of the appliance.13
Timing of Early Intervention
Class I
Usually problems in tooth size–arch length discrepancy presents at 8 years. Treatment is initiated after eruption of all incisors in lower arch and upper central incisors. Treatment started at early or late mixed dentition period is most beneficial compared to deciduous or permanent dentition period.14, 15
Class II
Waiting till late mixed dentition period is beneficial as greatest response to mandibular growth is seen during circumpubertal period for mandibular retro gnathic patients. Here functional appliance therapy directly followed by a phase of fixed therapy is considered ideal.14In presence of severe neuromuscular problem then treatment is started early mixed dentition period. In maxillary prognathism the treatment period is not crucial as extra oral traction can be used successfully in any of the later stages (late mixed/permanent dentition). In Class II patients with intra-arch problems, treatment can be initiated in 6-8 years to correct spacing, crowding, flaring using serial extraction or expansion appliances. But therapy to correct retrognathism has to be postponed to late mixed dentition period.
Class III
If diagnosed earlier in late deciduous dentition period treatment can be initiated immediately. Timing should be coincident with loss of upper deciduous incisors and eruption of permanent incisors. There might be more than one period of intervention in the mixed dentition.16
Summary and Conclusion
Different functional appliance designs act in variable manners and are not directly relatable. Considerable changes in appliance action such as the needed degree of required mandibular advancement, construction bites, and recommended time of wear brings about variable results. The duration of treatment differs for every individual person. Comparisons in relation to sex, age, and control between adequate research groups is lacking when long term controlled trials are done thereby misdirecting the reader about the possible and probable outcomes.1, 3
The results obtained with FR appliance are found to be engaging and meritorious. This proves beyond doubt or concern that interceptive treatment using FR appliance is functionally successful in rectifying the existent functional derangements. These outcomes can be regularly attained provided that the FR appliance is appropriately manufactured & handled as an effective exercise device.3 Evaluating the mechanisms of action for orthopaedic appliances is found to be advantageous for paediatric dentists who wants to maintain the achieved corrections in patients with mild Class II with mandibular retrognathism or mild Class III in relation to skeletal base.16 This acquaintance can thus yield clinically evident bone formation thereby inhibiting compressive action at the condyle-glenoid fossa interface, thus enabling uncomplicated growth pattern modifications in children.17
References
- Kannan A, Sathyanarayana HP, Padmanabhan S. Effect of functional appliances on the airway dimensions in patients with skeletal class II malocclusion: A systematic review. J Orthod Sci. 2017; 6(2):54-64.
CrossRef - Guimarães CH, Henriques JF, Janson G, Moura WS. Stability of interceptive/corrective orthodontic treatment for tooth ankylosis and Class II mandibular deficiency: A case report with 10 years’ follow-up. Indian Journal of Dental Research. 2015 May 1; 26(3):315.
CrossRef - Carrillo CM, Corrêa FN, Lopes NN, Fava M. Dental anomalies in children submitted to antineoplastic therapy. Clinics. 2014 Jun; 69(6):433-7.
CrossRef - Chadwick SM, Aird JC, Taylor PJ, Bearn DR. Functional regulator treatment of Class II division 1 malocclusions. The European Journal of Orthodontics. 2001 Oct 1; 23(5):495-505.
CrossRef - Almustaseb E, Jing M, Hong H, Bader R. The recent about growth modification using headgear and functional appliances in treatment of class II malocclusion: a contemporary review. IOSR- JDMS. 2014; 13(4):39-54.
CrossRef - Tanaka TG, Angelieri F, Kanashiro LK, Bommarito S. Stability evaluation of occlusal changes obtained with Fränkel's Function Regulator-2. Dental Press Journal of Orthodontics. 2012 Dec; 17(6):103-10.
CrossRef - Wahl N. Orthodontics in 3 millennia. Chapter 9: functional appliances to midcentury. Am J Orthod Dentofacial Orthop. 2006 Jun; 129(6):829-33.
CrossRef - Schmuth GP. Milestones in the development and practical application of functional appliances.Am J Orthod.1983 Jul; 84(1):48-53.
CrossRef - Huiskes R. If bone is the answer, then what is the question? J Anat. 2000; 197(2):145-56.
CrossRef - Fränkel R. Functional orthopedics American Journal of Orthodontics and Dentofacial Orthopedics. 2001 May 1; 119(5):11A.
CrossRef - Premkumar S. Textbook of craniofacial growth. JP Medical Ltd; 2011.
CrossRef - Woodside DG, Altuna G, Harvold E, Herbert M, Metaxas A. Primate experiments in malocclusion and bone induction. Am J Orthod 1983; 83:460.
CrossRef - Fränkel R. Orofacial orthopedics with the function regulator. S Karger Ag; 1989.
- Rajasekaran UB, Abdulla K. Interception of Skeletal Class 3 Malocclusion with Frankle 3 Appliance in Late Mixed Dentition.
- Shetti S, Golgire S, Patil A, Agrawal JA, Fulari SG. Management of Skeletal Class II Malocclusion with Functional Regulator II. Pediatr Dent Care. 2016; 1(118):2.
- Azamian Z, Shirban F. Treatment options for class III malocclusion in growing patients with emphasis on maxillary protraction. Scientifica. 2016; 2016.
CrossRef - Angelieri F, Franchi L, Cevidanes LH, Scanavini MA, McNamara Jr JA. Long-term treatment effects of the FR-2 appliance: a prospective evaluation 7 years’ post-treatment. European journal of orthodontics. 2013 Jun 4; 36 (2):192-9.
CrossRef





