.jpg)
Therapeutic Applications of Diode Lasers in Pediatric Dentistry: A Clinical Cases Series
Sharbari Dutta1*  , Abinash Mohapatra2 and Doyel Roy3
, Abinash Mohapatra2 and Doyel Roy3
1Department of Health Research, International Institute of Health Management Research, New Delhi, India .
2Department of Pedodontics and Preventive Dentistry, Kalinga Institute of Dental Sciences, KIIT University, Bhubaneswar, Orissa India .
3Department of Oral Medicine and Radiology, Dr. HSRSM Dental College and Hospital, Hingoli, Maharashtra India .
http://dx.doi.org/10.12944/EDJ.08.0109
Lasers have emerged as a revolutionary tool in dentistry. It offers precision, reduced bleeding, and enhanced patient comfort compared to conventional scalpel-based techniques. This case series presents four cases illustrating the management of various dental and oral conditions. Lasers have emerged as a highly effective, minimally invasive tool that fulfils these goals across a wide range of dental procedures. The laser-assisted approach resulted in a bloodless surgical field, minimal postoperative discomfort, and rapid healing. The case series reviews the classification and clinical applications of soft tissue lasers in modern dental practice.
Copy the following to cite this article:
Dutta S, Mohapatra A, Roy D. Therapeutic Applications of Diode Lasers in Pediatric Dentistry: A Clinical Cases Series. Enviro Dental Journal 2026;8(1).
DOI:http://dx.doi.org/10.12944/EDJ.08.0109Copy the following to cite this URL:
Dutta S, Mohapatra A, Roy D. Therapeutic Applications of Diode Lasers in Pediatric Dentistry: A Clinical Cases Series. Enviro Dental Journal 2026;8(1). Avialable here: https://bit.ly/4sRWAAQ
Download article (pdf) Citation Manager

Introduction
Lasers have become a revolutionary tool in dentistry. It is providing a more precise and comfortable alternative to traditional tools like scalpels and drills. Clinical evidence demonstrates that laser-assisted procedures have often led to reduced postoperative complications and faster recovery. It has made them a favourable choice in modern dental practice.1 The term LASER stands for Light Amplification by Stimulated Emission of Radiation.2 Its ability to coagulate blood vessels during surgery results in a bloodless operative field, minimising intraoperative and postoperative bleeding. This, in turn, lowers the risk of infection and inflammation.3
Since Maiman first introduced the laser to dentistry in 1960, its use has expanded dramatically across both hard- and soft-tissue procedures. Over the past two decades, research on dental laser applications has grown exponentially. In hard tissue procedures, lasers are utilised for caries prevention, tooth bleaching, removal and curing of restorative materials, cavity preparation, management of dentinal hypersensitivity, growth modulation, and diagnostic purposes. In soft tissue procedures, lasers play a vital role in promoting wound healing, excising hyperplastic tissue, uncovering impacted or partially erupted teeth, performing photodynamic therapy for malignant lesions, and photostimulating herpetic lesions. Furthermore, they are crucial for managing tissue prior to prosthetic work, such as achieving atraumatic gingival troughing for impressions and performing aesthetic crown lengthening.1,4
Recent case studies have demonstrated their efficacy in advanced procedures like second-stage implant uncovering and crown lengthening, where minimal bleeding and rapid healing are paramount for successful implant integration and aesthetics.5 The precision of laser cutting limits tissue damage, promoting faster recovery with less postoperative swelling and discomfort. Additionally, many laser-based soft tissue treatments require little to no local anaesthesia, improving patient comfort and compliance. This is especially relevant in paediatric dentistry, given its minimally invasive nature, making laser treatment well-suited for children who often exhibit dental fear and limited tolerance for conventional surgical interventions.6
Dentists are required to obtain informed consent before performing any laser procedure. Informed consent should clearly explain the purpose, benefits, potential risks, and alternative treatments, with parental consent mandatory for paediatric patients. Practitioners must undergo formal training and certification in laser use, as a lack of competence may constitute negligence. All equipment should meet recognised safety standards and be regularly maintained and calibrated. Protective measures, including wavelength-specific eyewear for patients and staff, are essential to prevent ocular or tissue injury. Accurate documentation of the procedure—detailing laser type, power settings, site treated, photographs, and postoperative outcomes—is legally important. Compliance with safety protocols, ethical conduct, and national regulations ensures that laser dentistry remains clinically effective while upholding patient welfare and practitioner protection.4
An 8-year-old female reported to the department with a painless swelling on the inner aspect of the lower lip. The patient was cooperative. No relevant family history found. The lesion was firm, smooth, and dome-shaped, measuring approximately 5 mm in diameter. Clinical diagnosis suggested an irritation fibroma caused by chronic lip biting. Later, the excised tissue was sent to the laboratory for confirmation. The reports confirmed fibroma. Oral fibromas are benign hyperplastic lesions caused by chronic irritation or trauma, frequently seen on the lips, buccal mucosa, and tongue. Laser excision provides a bloodless field, minimal postoperative pain, and rapid recovery, making it particularly advantageous in paediatric patients. (Figures 1-6).
Case 1: Laser Fibrotomy
 | Figure 1: Pre-operative picture showing fibroma in lower lip
|
 | Figure 2: Soft tissue Laser used for removal of fibroma
|
 | Figure 3: Fibrous tissue removed
|
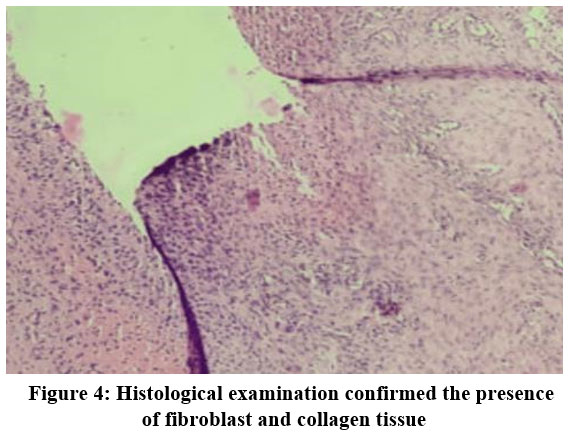 | Figure 4: Histological examination confirmed the presence of fibroblast and collagen tissue
|
 | Figure 5: Post Operative View
|
 | Figure 6: Post Operative View after 2 months of follow up
|
Treatment Procedure
After parental consent, the lesion was planned for removal using the Biolase Epic X soft-tissue diode laser. The surgical site was cleaned and isolated. Local anaesthesia (2% lignocaine with adrenaline 1:100,000) was administered. Excision was performed using a diode laser (Biolase Epic X, wavelength 940 nm, 400 µm tip, 1.2 W continuous mode). The lesion was excised circumferentially with excellent haemostasis and no need for sutures. The excised specimen was stored in 10% formalin for histopathological analysis in the laboratory. The laboratory results confirmed irritation fibroma. Excellent haemostasis was observed, and no sutures were required.
Postoperative Evaluation
The patient was prescribed mild analgesics and was advised to maintain oral hygiene. Follow-up showed healing by secondary intention at 7 days, complete epithelialization at 1 month, and no recurrence or scarring at 2 months.
Case Report 2: Laser-Assisted Pulpotomy in a Primary Molar
A 4-year-old female patient reported to the department with dental caries in a lower primary molar. The child was cooperative, and her medical history was non-contributory. Clinical and radiographic examination revealed a deep carious lesion involving the pulp without any signs of periapical pathology. Based on the diagnosis of reversible pulpitis, a pulpotomy procedure was planned using a diode laser. (Figures 7-18).
Case 2: Pulpotomy Done With Laser
 | Figure 7: Pre-operative intraoral view- Upper arch
|
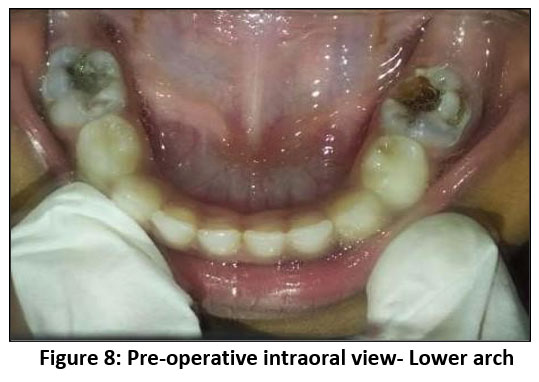 | Figure 8: Pre-operative intraoral view- Lower arch
|
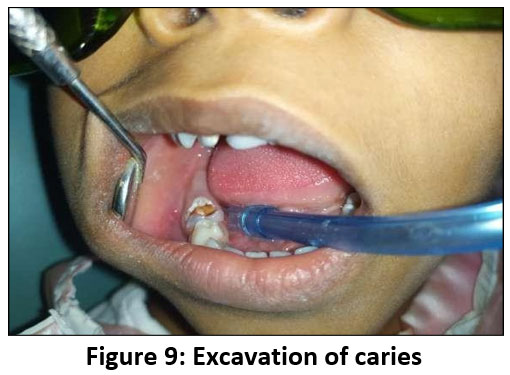 | Figure 9: Excavation of caries
|
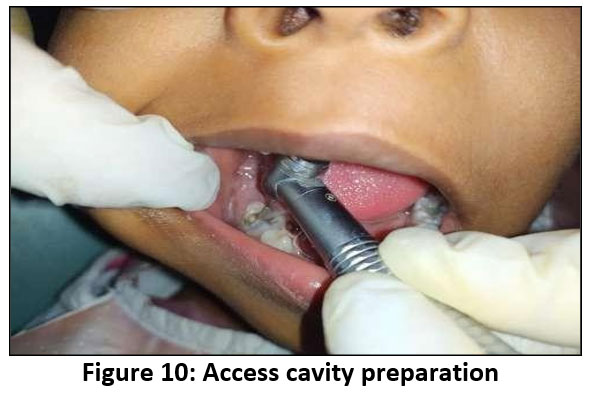 | Figure 10: Access cavity preparation
|
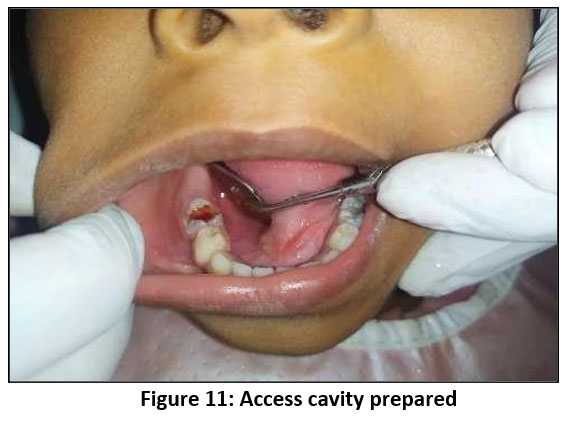 | Figure 11: Access cavity prepared
|
 | Figure 12: LASER assisted pulpotomy performed – Lateral view
|
 | Figure 13: LASER assisted pulpotomy performed – Frontal view
|
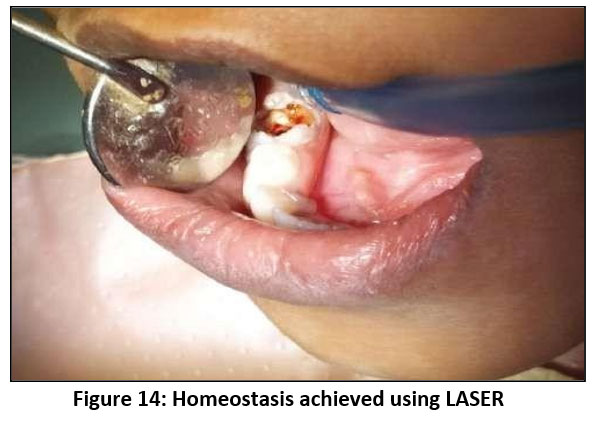 | Figure 14: Homeostasis achieved using LASER
|
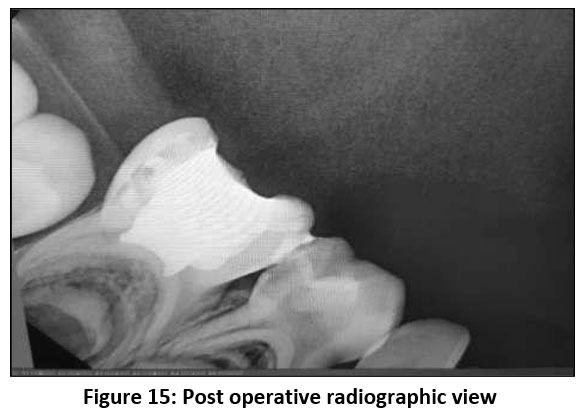 | Figure 15: Post operative radiographic view
|
 | Figure 16: Post operative clinical view
|
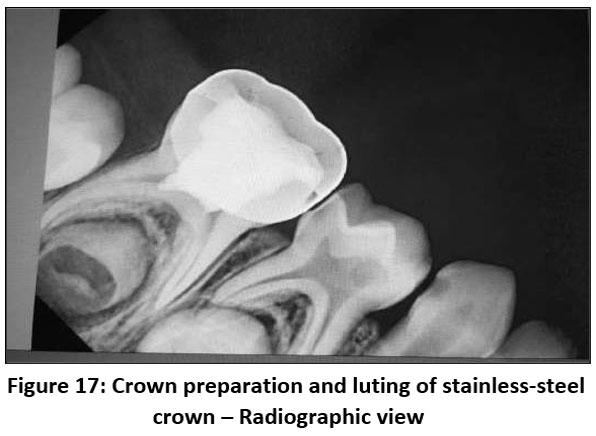 | Figure 17: Crown preparation and luting of stainless-steel crown – Radiographic view
|
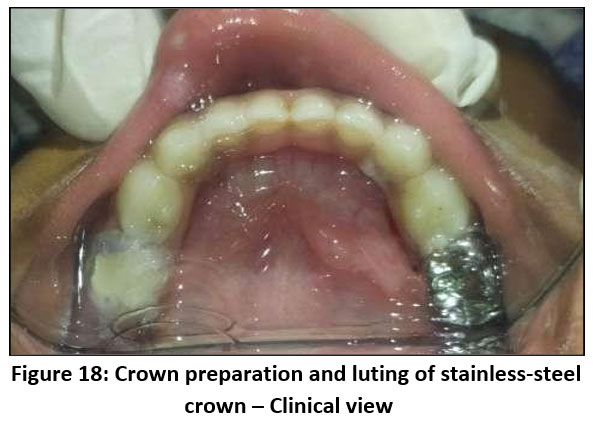 | Figure 18: Crown preparation and luting of stainless-steel crown – Clinical view
|
Treatment Procedure
Carious dentin was completely excavated to expose the coronal pulp, and hemostasis was achieved using a soft-tissue diode laser (Biolase Epic X) operating at a wavelength of 940 nm and power of 1.0–1.2 W in continuous mode. The coronal pulp tissue was removed under laser irradiation, which simultaneously provided decontamination and coagulation, resulting in a dry, blood-free field. The access cavity was then cleaned, and a suitable medicament base was placed over the pulp stumps. The tooth was subsequently restored with a stainless steel crown (SSC), which was fabricated and luted to restore the tooth’s form and function. The procedure was completed without any intraoperative complications, and the patient reported no discomfort. Postoperative instructions were given, and the patient was followed up clinically and radiographically.
Postoperative Evaluation
The immediate outcome showed an asymptomatic tooth with an intact restoration, while at the one-month follow-up, the tooth exhibited normal function, absence of pain, and radiographic evidence of maintained periradicular health. The result demonstrated a well-adapted crown and satisfactory pulpal healing, confirming the effectiveness of laser-assisted pulpotomy in paediatric dental management.
Case Report 3: Laser-Assisted Excision of Oral Mucocele
A 10-year-old female patient presented with a soft, fluctuant swelling on the lower lip. The lesion was asymptomatic and interfered slightly with speech and mastication. The patient was cooperative. No relevant family history found. Clinical findings were consistent with a mucocele. Laboratory confirmation was necessary for the final diagnosis.
Oral mucoceles are common benign lesions of the minor salivary glands, often resulting from ductal rupture or blockage. Conventional surgical excision carries risks of bleeding and recurrence. Laser excision ensures precise removal with minimal trauma and faster recovery. (Figures 19-24).
 Case 3: Removal of Mucocoele Using Laser
Case 3: Removal of Mucocoele Using Laser
 | Figure 19: Pre-operative picture showing mucocele in lower lip.
|
 | Figure 20: LASER removal of mucocele.
|
 | Figure 21: Excision of mucocele tissue.
|
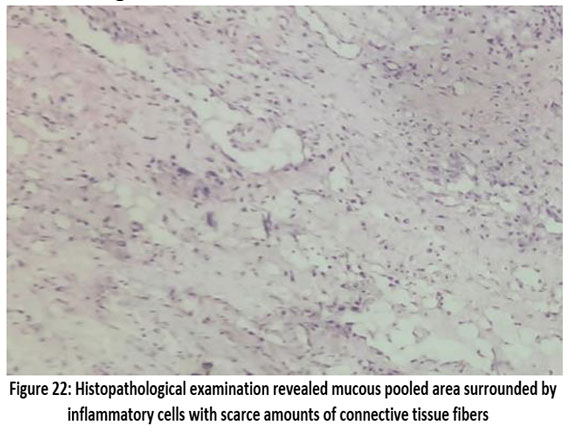 | Figure 22: Histopathological examination revealed mucous pooled area surrounded by inflammatory cells with scarce amounts of connective tissue fibers.
|
 | Figure 23: Post-operative view.
|
 | Figure 24: Post-operative view after 1 month
|
Treatment Procedure
The surgical area is cleaned and prepared. Under local anaesthesia, the lesion was excised using a diode laser (Biolase Epic X) at 0.8–1.2 W in continuous-contact mode. The lesion was ablated in layers until complete excision was achieved with minimal bleeding. The tissue was preserved for histopathological confirmation, verifying the diagnosis of mucocele. No sutures were required; homeostasis was instantaneous.
The excised tissue was sent for laboratory diagnosis, where it was confirmed to be a mucocele.
Postoperative Evaluation
The patient was reviewed after 1 week and 1 month. Healing was uneventful, with normal mucosal texture restored and no recurrence observed. The diode laser enabled a precise, bloodless, and comfortable surgical experience.
Case Report 4: Laser-Assisted Management of Recurrent Oral Erythema Multiforme in a Pediatric Patient
A 12-year-old male reported to the Department of Pedodontics with recurrent painful ulcers in the oral cavity for the past 6–7 months. Clinical examination of the mouth enabled identification of characteristic small, painful blisters or ulcers on the gums, tongue, or palate. The patient was cooperative. No relevant family history found. The lesions interfered with eating and speaking. The patient was initially evaluated and had complaints of persistent oral ulcerations for 6 months. (Figures 25-41).
Case 4: Laser Treatment Of Herpes Stomatitis
 | Figure 25: Pre-operative extraoral view
|
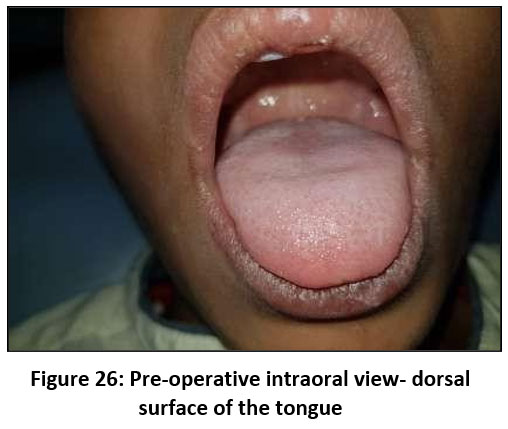 | Figure 26: Pre-operative intraoral view- dorsal surface of the tongue
|
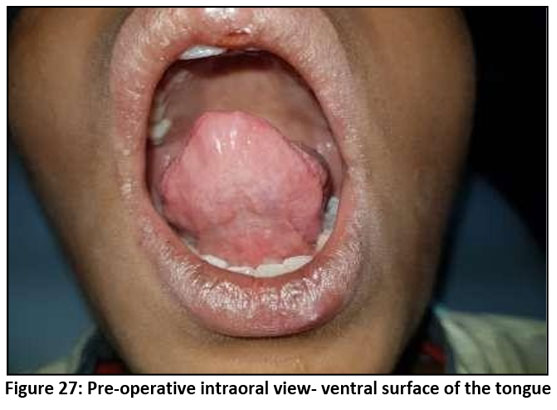 | Figure 27: Pre-operative intraoral view- ventral surface of the tongue
|
 | Figure 28: Pre-operative intraoral view- inner lip
|
 | Figure 29: Pre-operative intraoral view- right buccal surface
|
 | Figure 30: Pre-operative intraoral view- right buccal surface
|
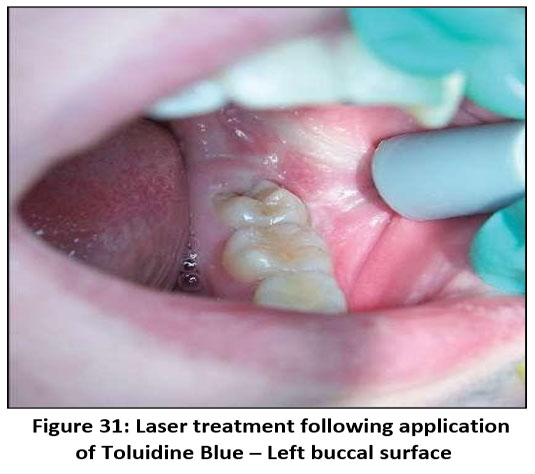 | Figure 31: Laser treatment following application of Toluidine Blue – Left buccal surface
|
 | Figure 32: Laser treatment following application of Toluidine Blue – Right buccal surface
|
 | Figure 33: Laser treatment following application of Toluidine Blue –lips
|
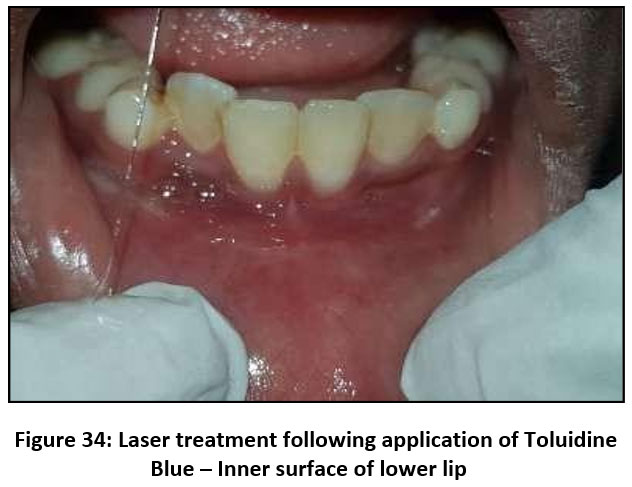 | Figure 34: Laser treatment following application of Toluidine Blue – Inner surface of lower lip
|
 | Figure 35: Toluidine Ointment
|
 | Figure 36: Post operative pictures after laser treatment activated with toluidine blue: Extraoral view
|
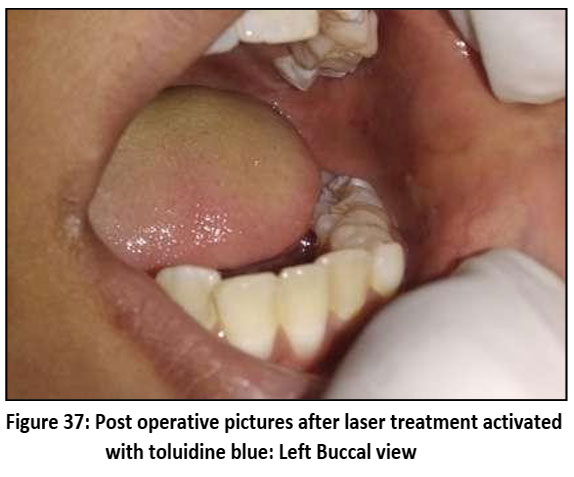 | Figure 37: Post operative pictures after laser treatment activated with toluidine blue: Left Buccal view
|
 | Figure 38: Post operative pictures after laser treatment activated with toluidine blue: Right Buccal view
|
 | Figure 39: Post operative pictures after laser treatment activated with toluidine blue: Lips
|
 | Figure 40: Post operative pictures after laser treatment activated with toluidine blue: Inner surface of the lower lips
|
 | Figure 41: Post operative pictures after laser treatment activated with toluidine blue: Inner surface of the upper lips
|
Treatment Procedure
Differential diagnoses included
Allergic stomatitis,
Herpetic stomatitis
Erythema multiforme
Acute necrotizing gingivostomatitis
Cytomegalovirus ulceration
Traumatic aphthous ulcers.
A Tzanck smear was performed, which showed no multinucleated giant cells. Herpetic gingivostomatitis is usually diagnosed clinically based on the patient’s history and the appearance of the oral lesions. The presence of typical vesicles and ulcers in the mouth is often enough for the clinician to make the diagnosis. However, when confirmation is needed, additional tests can be performed. Direct immunofluorescence testing of scrapings from the ulcer or of blister fluid can help confirm the infection. A Tzanck smear may also be used; this test can show the cellular changes caused by herpesvirus infection, but it cannot reliably differentiate between herpes simplex virus types 1 and 2 or varicella-zoster virus. The most definitive method of diagnosis is viral isolation through tissue culture. Antibody tests may show that the body has developed a response to the virus, but they cannot by themselves confirm the diagnosis. He was prescribed 400 mg acyclovir twice daily for 3 days, benzocaine gel, and vitamin B-complex for 1 month.
After a two-month follow-up, the ulcers recurred within three days of stopping antiviral therapy. The diagnosis was revised to recurrent herpetic stomatitis, and long-term acyclovir 200 mg twice daily again for 1 month, and topical mupirocin were prescribed. After 4 months of treatment, the patient was referred for paediatric evaluation. He had been on acyclovir therapy for one month, yet continued to have recurrent mucosal lesions. The paediatrician noted multiple 3-mm ulcerations on the labial gingiva and buccal mucosa and referred the patient to the Department of Oral Medicine for further evaluation.
Initial management included systemic therapy with:
Hesperidin 400 mg – one tablet four times daily for 7 days Omnacortil 20 mg – one tablet twice daily for 7 days
After the reduction of acute inflammation, laser therapy was initiated using a Biolase Epic X soft-tissue diode laser (940 nm wavelength, 1.0 W continuous mode, 400 µm tip). The lesions were stained with toluidine blue for precise localisation, followed by non-contact laser ablation and biostimulation of the affected mucosa under topical anaesthesia.
Postoperative Evaluation
Postoperative care included chlorhexidine mouthwash and application of topical anaesthetic gel. The patient was advised to maintain oral hygiene and avoid spicy food.
During the 1-week follow-up, there was a marked reduction in pain and erythema. By 2 weeks, complete epithelial healing was observed without scarring. At 1 month, the mucosa appeared normal with no recurrence of lesions.
The procedure was well tolerated, painless, and bloodless, with excellent patient comfort and cooperation.
Discussion
The present case series highlights the expanding role of diode lasers in pediatric dentistry, demonstrating their versatility across a wide spectrum of clinical applications ranging from
soft tissue surgery and pulp therapy to photobiomodulation. The findings highlight that the diode laser is minimally invasive, efficient, and child-friendly for managing oral conditions, aligning with the contemporary emphasis on atraumatic dental care in children.
Across all cases, the diode laser (940 nm) consistently provided excellent haemostasis, which can be attributed to its strong absorption by haemoglobin and pigmented tissues. This property results in effective coagulation of small blood vessels during incision and excision, creating a bloodless surgical field. Such an environment not only improves visibility for the operator but also significantly reduces operative time—an important consideration in paediatric patients with limited attention spans and heightened anxiety. The absence of sutures and minimal postoperative discomfort observed in Cases 1 and 3 corroborate previous reports that laser-assisted soft tissue surgery promotes faster epithelialisation and scar-free healing compared with conventional scalpel techniques.7
In Case 1, laser excision of irritation fibroma demonstrated precise tissue removal with minimal collateral damage. The ability of diode lasers to simultaneously ablate tissue and sterilize the surgical site likely contributed to the uneventful healing and absence of
postoperative complications. Similar outcomes have been documented in the literature, where diode lasers have shown superior control over intraoperative bleeding and reduced
postoperative oedema when compared with electrocautery, which is associated with greater thermal damage and delayed healing.8
The use of diode laser pulpotomy in Case 2 further emphasises its potential in vital pulp therapy for primary teeth. Effective haemostasis and decontamination of the pulp chamber are critical determinants of pulpotomy success. The laser’s bactericidal effect, combined with reduced mechanical trauma to the pulp tissue, may enhance favourable healing responses and maintenance of pulpal vitality. Additionally, the shortened treatment time and absence of rotary instrumentation improved patient cooperation, reinforcing the laser’s value as a behaviour-friendly adjunct in paediatric endodontic procedures.9
Case 3, involving excision of a mucocele, reinforces the diode laser’s suitability for managing benign soft tissue lesions in children. Although irritation fibroma and mucocele may present with similar clinical features—particularly as painless swellings of the lower lip in paediatric patients—their etiopathogenesis and biological behaviour differ significantly.
Irritation fibroma represents a reactive, non-neoplastic fibrous hyperplasia arising from chronic mechanical trauma such as lip biting, resulting in excessive collagen deposition and a firm, well-circumscribed lesion. In contrast, a mucocele is a mucus extravasation phenomenon caused by trauma to minor salivary gland ducts, leading to pooling of saliva within the connective tissue and a soft, fluctuant swelling with a bluish or translucent appearance. Histopathologically, fibroma is characterized by dense collagenised connective tissue covered by stratified squamous epithelium, whereas mucoceles show mucin-filled spaces surrounded by granulation tissue and inflammatory cells. Accurate differentiation between these lesions is essential, as their management strategies and recurrence potential differ; mucoceles require removal of adjacent minor salivary glands to prevent recurrence. while fibromas necessitate elimination of the chronic irritant. Laser-assisted excision offers precise and effective modality for both lesions, enabling minimal tissue trauma, excellent haemostasis, and rapid healing, which is particularly advantageous in pediatric patients where cooperation and postoperative comfort are critical.10,11
The lack of recurrence and rapid mucosal healing observed are consistent with studies reporting high success rates for laser excision of mucoceles due to precise targeting and minimal disruption of surrounding tissues. Compared with CO? lasers, which are also effective for such lesions, diode lasers offer the advantages of compact size, lower cost, and fibre-optic delivery, making them more accessible in routine clinical practice.12
Beyond surgical applications, Case 4 highlights the therapeutic role of lasers through photobiomodulation in managing recurrent oral erythema multiforme. Low-level laser therapy has been shown to exert anti-inflammatory, analgesic, and biostimulatory effects by enhancing cellular metabolism, promoting angiogenesis, and modulating inflammatory mediators. The rapid pain relief, accelerated healing, and sustained remission observed in this case support existing evidence advocating photo-biomodulation as a non-pharmacological adjunct or alternative in the management of painful oral mucosal disorders, particularly in pediatric patients where long-term medication use may be undesirable.13
In addition to these applications, laser technology has gained prominence in advanced infection management. In periodontal therapy, lasers are used either as a standalone modality or as an adjunct to conventional debridement, enabling direct targeting of pathogenic bacteria within deep periodontal pockets. This precise microbial reduction limits systemic dissemination and supports long-term periodontal stability. Similarly, in endodontics, laser-assisted irrigation and disinfection enhance penetration into complex root canal anatomy and generate photoacoustic shockwaves within the irrigants, achieving superior canal sterilisation and reducing the risk of persistent infection and treatment failure.14
When considered alongside other dental lasers, the diode laser occupies a unique niche. While erbium lasers are preferred for hard tissue procedures due to their high absorption in hydroxyapatite and water, CO? lasers excel at precise superficial soft-tissue ablation. Diode lasers offer an optimal balance of efficacy, affordability, and ease of use for soft tissue management and phototherapy. Their limited interaction with hard tissues reduces the risk of inadvertent damage, further enhancing safety in paediatric settings.15
The case series includes different clinical indications (fibroma excision, pulpotomy, mucocele removal, and photobiomodulation for mucosal lesions). While this demonstrates the versatility of diode lasers, it limits the ability to draw conclusions about their effectiveness for any single specific paediatric dental condition. Although the postoperative outcomes were favourable, the follow-up period in the cases ranged from 1 week to 2 months, which may not be sufficient to evaluate long-term recurrence of lesions such as mucocele or irritation fibroma, or long-term success of pulpotomy procedures in primary teeth.
The cases majorly underline the diode laser as a reliable, versatile, and minimally invasive tool in paediatric dentistry. Its ability to enhance patient comfort, reduce operative stress, and promote favourable healing outcomes makes it a valuable addition to routine paediatric dental practice. Diode lasers are likely to play an increasingly integral role in delivering safe, efficient, and child-centred dental care.
Conclusion
In contemporary dental practice, achieving a bloodless operative field, minimal patient discomfort, and faster postoperative recovery are key objectives for both clinicians and patients. Lasers have emerged as a highly effective, minimally invasive tool that fulfils these goals across a wide range of dental procedures. Their precision, superior haemostasis, and bactericidal properties make them particularly advantageous in paediatric and soft-tissue surgeries, as well as in managing chronic and premalignant oral conditions such as oral submucous fibrosis (OSMF). Despite their proven clinical benefits, the literature still reports a lack of large-scale studies evaluating the long-term outcomes and comparative efficacy of different laser systems in such conditions. Therefore, further well-designed clinical trials are necessary to validate their broader therapeutic potential. Nevertheless, the integration of laser technology into routine dental practice should be encouraged, as it represents a safe, reproducible, and patient-friendly advancement in modern dentistry.
Acknowledgement
The authors sincerely thank the Kalinga Institute of Dental Sciences for facilitating access to patients and supporting the clinical aspects of this study. We are grateful to the International Institute of Health Research for providing essential resources that enabled the completion of this work. We also extend our appreciation to Dr. Jyotsna Rai, Research Officer, IIHMRD for her valuable contribution to the initial literature survey that guided the development of this manuscript.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article
Conflict of Interest
The authors do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval
Informed Consent Statement
Written informed consent was obtained from the patient for treatment and for the use of clinical information and images for academic publication. The patient’s identity has been kept confidential. As this manuscript is a case series with no experimental intervention, formal ethical committee approval was not required in accordance with institutional guidelines. All procedures were performed following accepted clinical standards.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to Reproduce Material from Other Sources
There are no such items which have been published earlier
Author Contributions
Sharbari Dutta: Conceptualization, Methodology, Writing – Original Draft, Data Collection, Analysis, Writing – Review & Editing.
Abinash Mohapatra Visualization, Supervision, Project Administration.
Doyel Roy: Data collection, clinical cases treatment.
References
- Sachelarie L, Cristea R, Burlui E, Hurjui LL. Laser Technology in Dentistry: From Clinical Applications to Future Innovations. Dentistry Journal. 2024;12(12):420. doi:10.3390/dj12120420
CrossRef - Kotb S. Photobiomodulation and Its Application in Dentistry. SSRN Journal. Published online 2023. doi:10.2139/ssrn.4338073
CrossRef - Liaqat S, Qayyum H, Rafaqat Z, et al. Laser as an innovative tool, its implications and advances in dentistry: A systematic review. Journal of Photochemistry and Photobiology. 2022;12:100148. doi:10.1016/j.jpap.2022.100148
CrossRef - Verma SK, Maheshwari S, Singh RK, Chaudhari PK. Laser in dentistry: An innovative tool in modern dental practice. National Journal of Maxillofacial Surgery. 2012;3(2):124-132. doi:10.4103/0975-5950.111342
CrossRef - Kaur M, Sharma YD, Singh P, Sharma S, Wahi A. Comparative evaluation of efficacy and soft tissue wound healing using diode laser (810 nm) versus conventional scalpel technique for second-stage implant surgery. J Indian Soc Periodontol. 2018;22(3):228. doi:10.4103/jisp.jisp_46_17
CrossRef - Alkari S, Hamadah O, Parker S. Comparison between the surgical scalpel and carbon dioxide laser in managing excessive gingival display using lip repositioning technique: a randomized controlled clinical study. Maxillofac Plast Reconstr Surg. 2025;47(1):20. doi:10.1186/s40902-025-00475-8
CrossRef - Bhatsange A, Meshram E, Waghamare A, Shiggaon L, Mehetre V, Shende A. A clinical and histological comparison of mucosal incisions produced by scalpel, electrocautery, and diode laser: A pilot study. J Dent Lasers. 2016;10(2):37. doi:10.4103/2321-1385.196962
CrossRef - Bhatsange A, Meshram E, Waghamare A, Shiggaon L, Mehetre V, Shende A. A clinical and histological comparison of mucosal incisions produced by scalpel, electrocautery, and diode laser: A pilot study. J Dent Lasers. 2016;10(2):37. doi:10.4103/2321-1385.196962
CrossRef - Afkhami F, Rostami G, Xu C, Walsh LJ, Peters OA. The application of lasers in vital pulp therapy: a review of histological effects. Lasers Med Sci. 2023;38(1):215. doi:10.1007/s10103-023-03854-7
CrossRef - Rangeeth B, Moses J, Reddy VK. A rare presentation of mucocele and irritation fibroma of the lower lip. Contemp Clin Dent. 2010;1(2):111. doi:10.4103/0976- 237X.68596
CrossRef - Piña A, Almeida L, Andrade BA, León J. Clear cell change in a lower lip mucocele. J Oral Maxillofac Pathol. 2013;17(2):318. doi:10.4103/0973-029X.119776
CrossRef - Sadiq MSK, Maqsood A, Akhter F, et al. The Effectiveness of Lasers in Treatment of Oral Mucocele in Pediatric Patients: A Systematic Review. Materials. 2022;15(7):2452. doi:10.3390/ma15072452
CrossRef - Fabre HSC, Navarro RL, Oltramari-Navarro PVP, et al. Anti-inflammatory and analgesic effects of low-level laser therapy on the postoperative healing process. J Phys Ther Sci. 2015;27(6):1645-1648. doi:10.1589/jpts.27.1645
CrossRef - Cai E, Beppler C, Eichorst J, Marchuk K, Eastman SW, Krummel MF. T cells use distinct topographical and membrane receptor scanning strategies that individually coalesce during receptor recognition. Proc Natl Acad Sci USA.2022;119(32):e2203247119. doi:10.1073/pnas.2203247119
CrossRef - Verma SK, Maheshwari S, Singh RK, Chaudhari PK. Laser in dentistry: An innovative tool in modern dental practice. National Journal of Maxillofacial Surgery. 2012;3(2):124-132. doi:10.4103/0975-5950.111342
CrossRef





